Weight Loss, Wellness & Beauty
Caring For Our Patients Since 2007
Our 4 Most Popular Weight Loss Products
We understand that when it comes to weight loss, finding the right solution can be challenging. That’s why we offer 4 highly effective weight loss treatments that you can order online:
HCG Weight Loss, Tirzepatide, Bella Phentermine, and Semaglutide for weight loss.
HCG
Human Chorionic Gonadotropin-
(2) 25 Day Diets Patients can expect to lose up to 1Lb. Day
-
DIET- Yes
-
No Exercise Required
-
RX- Required
-
Daily Injection
-
Dr. Consult Included
TIRZEPATIDE
Same Ingredient in MOUNJARO-
Monthly Program
Patients can expect to lose up to 2-3 lbs. per week. -
DIET- No
-
No Exercise Required
-
RX- Required
-
Weekly Injection
-
DR. Consult Included
SEMAGLUTIDE
Active Ingredient in WEGOVY-
Monthly ProgramPatient can lose Up to 1-2 lbs. per week.
-
DIET - No
-
Moderate Exercise
-
RX -Required
-
Weekly Injection
-
Dr. Consult Included
BELLA
FDA Approved Phentermine-
Monthly ProgramAppetite SuppressantVariable Weight Loss
-
DIET- No
-
Moderate Exercise
-
RX- Required
-
Daily Capsule
-
DR. Consult (After 1st Mo.)
- Weight Loss
- Diet
- Exercise
- Prescription
- Dosage
- Dr. Consultation
HCG
Human Chorionic Gonadotropin
Rapid Weight Loss
- (2) 25 Day Diets
Patients can expect to
lose up to 1Lb. Day - Yes
- No Exercise Required
- Required
- Daily Injection
- Included
TIRZEPATIDE
Same Ingredient in MOUNJARO
Quick Weight Loss
Monthly Program
Patients can expect
to lose up to 2-3 lbs. per week.- No
- No Exercise Required
- Required
- Weekly Injection
- Included
BELLA
FDA Approved Phentermine
Gradual Weight Loss
- Monthly Program
Appetite Suppressant
Variable Weight Loss - No
- Moderate
- Required
- Daily Pill
- Included
SEMAGLUTIDE
Active Ingredient in WEGOVY
Long-Term Weight Loss
- Monthly Program
Patient can lose Up to
1-2 lbs. per week. - No
- Moderate
- Required
- Weekly Injection
- Included
You will not be billed until you are approved for a prescription.
Tirzepatide
The service is impeccable with New Beginnings!
Excellent Service
Joleen and the team are always so friendly and responsive and I find their products to be very effective.
B12 Injections, LipoTropic Injections
So far I love my experience with new beginnings. I used them in 2018 and had great success, but 2020 with COVID I lost all control and gained the weight bac(…)
Bella Phentermine
You make it very easy to understand and to order. My husband and I are returning Patients for the 3rd or 4th time.
Thank you for your great customer service!
B12 Vitamin Injections
Knowledgeable and friendly. Joie is great. Highly recommend this company
Anti Fungal Solutions, B12 Vitamin Injections
Glutathione Injections, LipoTropic Injections
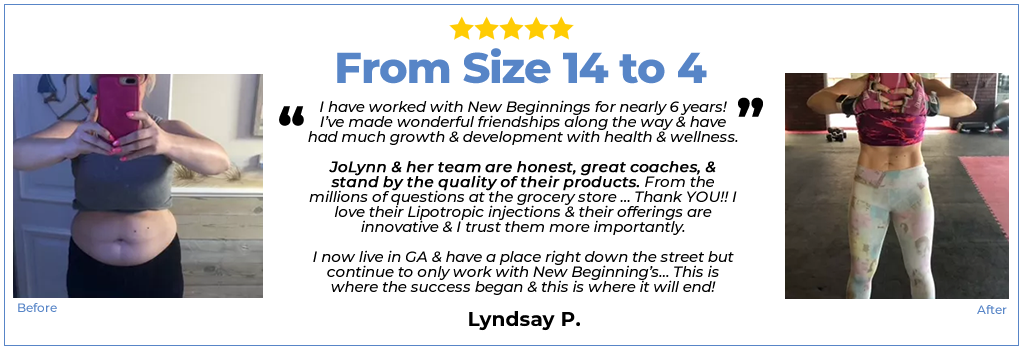
I have worked with New Beginnings for nearly 6 years! I’ve made wonderful friendships along the way &(…)
Glutathione Injections, LipoTropic Injections
Hello, I am still a beginner, however positive results are definitely happening. I have noticed my hair looking better, my nails are a lot stronger,(…)
B12 Vitamin Injections, LipoTropic Injections
Been a New Beginnings customer for 5 yrs and hands down they are THE BEST. I’ve never been disappointed in treatments, products. Not too mention, (…)
Bella Phentermine
Joie in Customer Service was lovely to work with. She answered all my questions and made sure I understood the ordering process and scheduled my doctor phone consult. Dr. Zel(…)
BELLA
Bella is a weight loss pharmaceutical product that is available with or without Phentermine is a prescription medication that helps suppress your appetite. Phentermine has been utilized for weight loss for over 50 years and is still considered one of the most effective weight loss medications. When Bella is ordered with or without Phentermine through New Beginnings Medical, you are getting a high quality medication that will help you achieve your weight loss goals.as
SEMAGLUTIDE
TRIZEPATIDE

Need Help Deciding Which Is Best For You?
Call now and experience a truely personal approach to Telehealth!
WE HELP MEN AND WOMEN
LOOK AND FEEL GREAT

LIPOTROPICS

VITAMIN D

NAD+ Injection

Vitamin C Injection

B12 Injections

GlutithionE

Simple 3 Step Process

Order
Select a product that meets your needs, then use our secure platform to safely checkout .

Consultation
A licensed Medical Doctor in your State will discuss, approve & order your prescription medicine.

Delivered
Approved products are shipped to your residence from a licensed U.S. Pharmacy.
Tirzepatide
The service is impeccable with New Beginnings!
Excellent Service
Joleen and the team are always so friendly and responsive and I find their products to be very effective.
B12 Injections, LipoTropic Injections
So far I love my experience with new beginnings. I used them in 2018 and had great success, but 2020 with COVID I lost (…)
Bella Phentermine
You make it very easy to understand and to order. My husband and I are returning Patients for the 3rd or 4th time.
Thank you for your great customer service!
B12 Vitamin Injections
Knowledgeable and friendly. Joie is great. Highly recommend this company
Anti Fungal Solutions, B12 Vitamin Injections
Glutathione Injections, LipoTropic Injections
I have worked with New Beginnings for nearly 6 years! I’ve made (…)
Glutathione Injections, LipoTropic Injections
Hello, I am still a beginner, however positive results are definitely happening. I have noticed my hair looking (…)
B12 Vitamin Injections, LipoTropic Injections
Been a New Beginnings customer for 5 yrs and hands down they are THE BEST. I’ve never been disappointed in (…)
Bella Phentermine
Joie in Customer Service was lovely to work with. She answered all my questions and made sure I understood the ordering process and (…)
Typical Weight Loss FAQ's
When you order from New Beginnings Medical, you can trust that you are getting the highest quality care and treatment available. We are dedicated to helping you achieve your weight loss goals and improving your overall health and well-being. Our medical team is comprised of experienced doctors who specialize in weight loss, and we use only the most advanced and effective treatments to help you succeed.
So, whether you’re looking to buy HCG online, order Bella Phentermine online, or purchase Semaglutide online, New Beginnings Medical is here to help. With our personalized treatment plans and high-quality medications, you can achieve the results you’ve always wanted and start living your best life. Order now and start your journey to a healthier, happier you!